Tree in Lung: Causes, Symptoms, and Treatment Explained
A “tree in lung” refers to a branching pattern of pulmonary blood vessels that looks like tree limbs when seen on imaging scans. It’s not a literal tree, but it precisely describes how pulmonary arteries or veins appear when blood flow is compromised—often due to clots or vascular issues. This visual cue helps doctors spot potentially serious problems quickly.
Why the “Tree” Metaphor in Lungs Matters
When radiologists mention a tree-like pattern in the lungs, they’re usually referring to pulmonary embolism (PE) or pulmonary arteriovenous malformation (PAVM). In PE, a clot blocks an artery, cutting off blood flow beyond the blockage. This causes the vessel to abruptly end, mimicking a tree branch that’s snapped off. It’s such a distinct look that the term “vascular cutoff sign” is often used. The image instantly screams—look here, something’s blocked.
On the other hand, PAVM involves abnormal connections between arteries and veins, bypassing the capillaries—creating intricate, tangled patterns that also resemble tree branches. These malformations can develop over time and make the lung look like a dense thicket under a scan.
Understanding Causes: Pulmonary Embolism vs. Vascular Malformation
Pulmonary Embolism (PE)
PE is the most common reason for the tree-in-lung appearance. Here’s how it happens:
- A clot usually forms in the deep veins of the leg (deep vein thrombosis, or DVT).
- The clot breaks off and travels through the bloodstream to the lungs.
- It lodges in a pulmonary artery, abruptly stopping blood flow—and that creates that tree branch “cutoff” look on a CT angiogram.
- Sometimes, multiple clots cause a more complex pattern.
Pulmonary Arteriovenous Malformation (PAVM)
PAVMs are congenital or acquired irregular connections between arteries and veins in lungs. They’re less common than PE but significant:
- Genetic factors (like hereditary hemorrhagic telangiectasia) often play a role.
- These connections allow blood to pass without oxygenation—leading to low oxygen levels and potentially dangerous complications like stroke.
- Under imaging, PAVM appears as a dense network, again resembling branches and twigs of a tree.
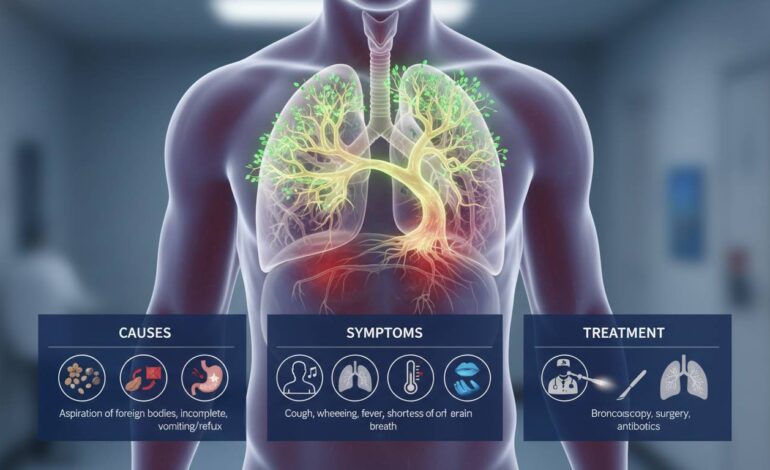
Recognizing Symptoms Linked to the “Tree in Lung” Look
For Pulmonary Embolism
Symptoms often come on suddenly:
- Shortness of breath that’s unexpected and intense.
- Chest pain, especially when breathing deeply.
- Fast heartbeat or feeling lightheaded.
- Sometimes collapse or coughing up blood.
For PAVM
Symptoms are often subtler and chronic:
- Low blood oxygen, leading to fatigue or increased breathlessness over time.
- Risk of stroke or brain abscess because of deoxygenated blood slipping through bypasses.
- Occasional coughing up blood.
- Frequently found when investigating unexplained low oxygen or neurological events.
How the Diagnosis Gets Made: Imaging and Tests
Computed Tomography Pulmonary Angiography (CTPA)
CTPA is the gold standard. For PE, it shows abrupt vessel cut-offs—even small ones. For PAVM, it outlines tangled vessel masses. This scan is fast, widely available, and usually first-line.
Ventilation-Perfusion (V/Q) Scan
Used when CTPA is not ideal (e.g., poor kidney function or contrast allergy). It highlights areas that aren’t getting proper blood flow. A mismatch between ventilation and perfusion is a big red flag for PE.
Contrast Echocardiography and MRI
For PAVM, a contrast echo or MRI can help spot abnormal shunts. These tests are especially helpful when genetic conditions or subtle abnormalities are suspected.
Lab Tests and Further Evaluation
- D-dimer test helps rule out PE when combined with clinical risk scores.
- Oxygen levels, blood gases, and genetic testing (for suspected PAVM syndromes) guide further assessment.
Treatment Pathways: From Emergencies to Long-Term Control
Managing Pulmonary Embolism
- Immediate anticoagulation – Blood thinners like heparin or direct oral anticoagulants (DOACs) to stop clot growth.
- Clot removal in severe cases – In high-risk or unstable patients, doctors may use clot-busters (thrombolytics) or surgical/endovascular removal.
- Ongoing care – Long-term blood thinners and monitoring for recurrence. In rare cases, placement of inferior vena cava (IVC) filters helps prevent future clots.
Dealing with Pulmonary Arteriovenous Malformation
- Embolotherapy (least invasive) – A catheter is used to place coils or plugs to seal off the abnormal vessels.
- Surgical removal – Reserved for large or hard-to-access malformations.
- Surveillance and follow-up – Repeat imaging, especially in genetic conditions, to catch any new lesions early.
Real-World Case Snippets
- A middle-aged man collapsed after a flight. CTPA showed a sharp cutoff in a pulmonary artery—classic tree-in-lung. He was treated quickly with anticoagulants, then switched to a DOAC, and recovered well.
- A woman with mild shortness of breath and unexplained low oxygen. Imaging discovered a small PAVM. Embolization helped immediately, and her oxygen levels went up. She later joined a hereditary hemorrhagic telangiectasia support group.
- A patient with recurrent strokes and no carotid disease. Contrast echo flagged a right-to-left shunt. Further imaging found a hidden PAVM. Closing it stopped the brain events.
Why It Helps to Think Like a Radiologist
Radiologists literally map the lung’s vascular tree. When a branch suddenly disappears, alarm bells ring—not in a spooky way but in a lifesaving one. Recognizing that pattern quickly can change outcomes dramatically. It’s visual, intuitive, yet grounded in solid pathology.
Challenges and Considerations
Mimics and Pitfalls
- Sometimes tumors or infections narrow vessels—not an embolus.
- Artifacts on scans can mislead toward a false tree-like appearance.
- For PAVM, small lesions may hide or mimic other nodules.
Follow-up Importance
- After treating a PE, doctors check whether clots are gone and adjust long-term plans.
- PAVM patients often need periodic imaging—even years later—to catch new growths.
Prevention and Patient Awareness
- Healthy habits to reduce clot risk—move frequently during long journeys, stay hydrated, manage weight and blood pressure.
- Patients with known genetic risks (like hereditary hemorrhagic telangiectasia) benefit from regular monitoring and early treatment when new vascular lesions appear.
- A single phrase on a scan—“tree in lung”—should prompt prompt attention and well-informed follow-up.
Advanced Insights for Clinicians
When to Suspect PE vs. PAVM
- Acute symptoms like chest pain or rapid shortness of breath usually point to PE.
- Otherwise unexplained hypoxia, paradoxical brain events, or family history may signal PAVM.
Linking Imaging to Physiology
- In PE, the blocked branch means that portion of lung isn’t getting blood—oxygen and carbon dioxide exchange collapses.
- PAVM creates a bypass—oxygen-poor blood goes straight to veins, escaping gas exchange, and often complicates with oxygen desaturation and stroke risk.
Tips for Patients and Providers
- Quick recognition of worrisome patterns on imaging saves lives.
- Short-term and long-term planning differ: manage immediate threats like PE, plan ahead for PAVM surveillance.
- Clear communication: explaining the “tree in lung” in plain terms helps patients understand the urgency or nature of the issue.
- Team approach: collaboration between radiology, pulmonology, cardiology, genetics, surgery ensures well-rounded care.
Conclusion
The “tree in lung” isn’t poetic—it’s clinical. It flags important vascular issues like PE or PAVM. Discerning between the two, diagnosing fast, and treating effectively can save lives and improve long-term outcomes. It’s a vivid reminder how imaging shapes real decisions, every day. It’s worth paying attention when a scan shows that branching silhouette—it matters.
FAQs
What does “tree in lung” mean in simple terms?
It describes how pulmonary blood vessels look on scans when they resemble branching tree limbs—usually due to blocked or malformed vessels.
Which condition is most commonly associated with this appearance?
Pulmonary embolism is the most frequent cause, marked by sudden vessel cutoff from a clot, creating that tree-branch look.
Can the “tree in lung” appear in other conditions?
Yes—pulmonary arteriovenous malformation (PAVM) can also create a branching network appearance, but it indicates abnormal vessel connections rather than clots.
How is a pulmonary embolism treated once this sign is seen?
Treatment typically starts with blood thinners (anticoagulation). In severe cases, clot removal or thrombolytic therapy may be needed.
What’s the long-term plan for someone with a PAVM?
Embolization or surgery to block abnormal vessels is common. Patients often undergo periodic imaging to monitor for new malformations.
Is “tree in lung” an emergency sign?
It can be. Especially for pulmonary embolism, the branching cutoff suggests possible life-threatening blockage—prompt evaluation is crucial.